Introduction
Physical therapy in Delray Beach for Pediatric Issues
Welcome to Miller PT's resource about Clubfoot.
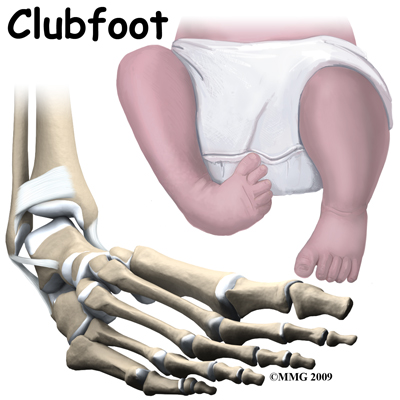 Clubfoot is a congenital condition that affects newborn infants. The medical term for clubfoot is Congenital Talipes Equinovarus. This condition has been described in medical literature since the ancient Egyptians. Congenital means that the condition is present at birth and occurred during fetal development. The condition is not rare and the incidence varies widely among different races. In the Caucasian population, about one in a thousand infants are born with a clubfoot. In Japan, the numbers are one in two thousand and in some races in the South Pacific it can be as high as seven infants in one thousand who are born with a clubfoot. The condition affects both feet in about half of the infants born with clubfoot. Clubfoot affects twice as many males as females.
Clubfoot is a congenital condition that affects newborn infants. The medical term for clubfoot is Congenital Talipes Equinovarus. This condition has been described in medical literature since the ancient Egyptians. Congenital means that the condition is present at birth and occurred during fetal development. The condition is not rare and the incidence varies widely among different races. In the Caucasian population, about one in a thousand infants are born with a clubfoot. In Japan, the numbers are one in two thousand and in some races in the South Pacific it can be as high as seven infants in one thousand who are born with a clubfoot. The condition affects both feet in about half of the infants born with clubfoot. Clubfoot affects twice as many males as females.
This guide will help you understand:
- what part of the foot is involved
- what causes the condition
- what treatment options are available
- what Miller PT's approach to rehabilitation is
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Pediatrics|limit:15|heading:Hear from some of our *Pediatrics* patients#
Anatomy
What part of the foot is affected?
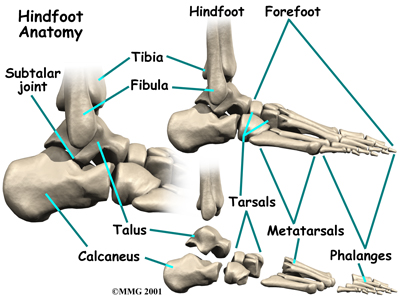
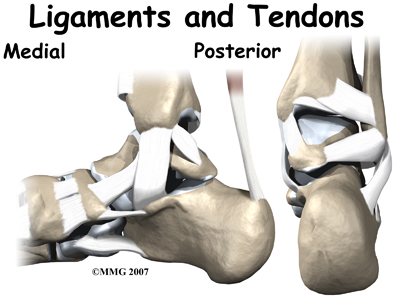
The tarsal bones are the seven bones that make up the heel and the midfoot. The metatarsals and the phalanges are connected to the tarsals and form the forefoot. Clubfoot primarily affects three bones: the calcaneus, talus and navicular. The deformity can affect the growth of the entire foot to some degree so other bones may be involved as well.
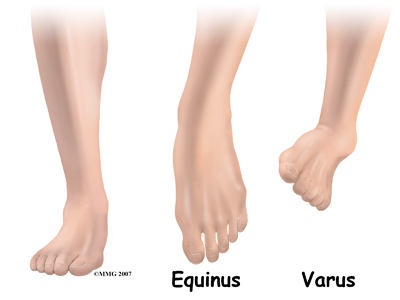
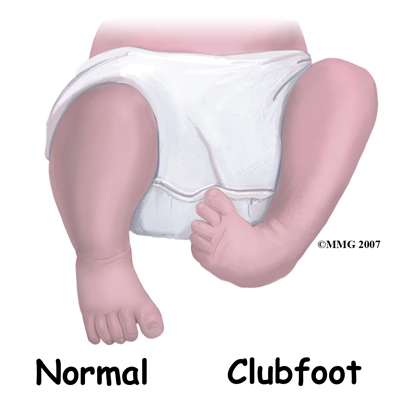
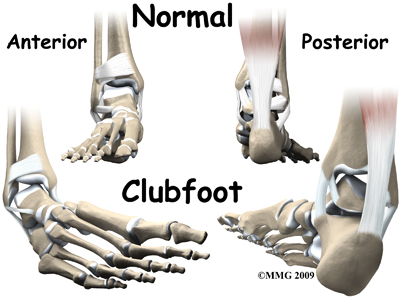
The clubfoot is unmistakable. The foot is turned under and towards the other foot. The medical terminology for this position is equinus and varus. Equinus means that the toes are pointed down and the ankle flexed forward (sort of like the position of the foot when a ballet dancer is on her toes). Varus means tilted inward. The ankle is in varus position when you try to put the soles of your feet together.
This twisted position of the foot causes several problems in the foot. The ligaments, which are the connecting tissue between the bones, are contracted, or shortened and the joints between the tarsal bones do not move, as they should. The bones themselves are deformed. This results in a very tight stiff foot that cannot be placed flat on the ground for walking. To walk, the child must walk on the outside edge of the foot rather than on the sole of the foot.
One interesting finding is that the calf muscles on the leg with the clubfoot are smaller than normal. If the clubfoot only affects one foot, the calf muscles on this leg will always remain smaller than the opposite side.
Causes
How does this problem develop?
During the nine months of pregnancy, the fetus undergoes remarkable changes. In the skeleton, these changes include the separation of each individual bone in the body from one mass of bone material. In some cases, this process is flawed. A clubfoot occurs when this failure of separation occurs in the tarsal bones of the foot.
Until recently, most experts believed that the clubfoot deformity was due to the foot being stuck in the wrong position in the womb. As development progressed, the foot could not grow normally because it was turned under and held in that position. Today, most information suggests that clubfoot is hereditary, meaning that it runs in families. It is not clear what genetic defect causes the problem. It is not known yet whether the defect affects the development of the muscles, blood vessels, or bones of the foot.
The foot is an incredibly complex structure. For the foot to grow and develop correctly, all of the bones of the foot must move normally in relationship to each other. If the movement between two bones is abnormal, or non-existent, that changes how the bones grow after birth. If untreated, over time this leads to further deformity in the foot.
Symptoms
What does this problem feel like?
The condition in itself is not painful to the child. The primary problem of a clubfoot is that the foot cannot be placed flat on the ground so that the child can walk on the sole of the foot. In developing countries where there is sometimes no treatment for conditions such as this, adults with a clubfoot walk on the side of their foot. They do not walk normally and this may cause pain. Due to this abnormal force on the side of the foot the foot is extremely deformed with calluses where it contacts the ground. Footwear is very difficult to fit and usually must be custom-made, as normal shoes will not fit. Eventually the abnormality can lead to wear and tear arthritis in the joints of the foot, pain, and decreased ability to walk.

Diagnosis
How do doctors identify the problem?
The history and physical examination make the diagnosis of clubfoot. The appearance alone is usually enough to determine that a clubfoot is present. A complete examination of the newborn with a clubfoot is critical since there are other genetic conditions that are associated with clubfeet. Your pediatrician will perform a complete evaluation to make sure there are no other congenital conditions to be concerned with.
A clubfoot can be diagnosed before birth using ultrasound. Many women have routine ultrasound tests to assess the status of the pregnancy. There is currently no treatment available before birth if a clubfoot should be found. Being that clubfoot is associated with other serious congenital and genetic abnormalities, the obstetrician may recommend amniocentesis to look for genetic problems in the fetus if a clubfoot is present. An amniocentesis is a test where a needle is inserted into the uterus and a small amount of fluid removed. This fluid is sent to the lab for analysis. If evidence for serious genetic or congenital anomalies is found, then the option of terminating the pregnancy exists.
X-rays are helpful in determining the severity of the condition. This information may become important later in trying to decide what treatment is best to recommend. Usually, no other imaging studies are needed.
Treatment
What treatment options are available?
Treatment for clubfoot usually begins at birth. Treatment in the majority of infants will require both non-surgical treatment and surgery. The foot will never be normal, but treatment can provide a very functional foot that can be used for walking without pain.
Nonsurgical Treatment
The most commonly used non-surgical treatment in the newborn and infant is manipulation and casting. This is started as soon as possible. The foot is manipulated to stretch and loosen the tight structures. The foot is then placed in a cast to hold it in a corrected position. This is repeated every one or two weeks until the deformity is corrected or surgery is performed.
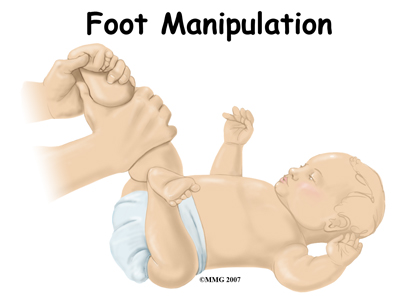

As any parent knows, the newborn grows rapidly after birth. The technique of manipulation and casting the foot is used to guide the growth of the foot towards the normal alignment. Without this guidance, the foot will remain deformed and may actually get worse. The greatest chance for correction of deformity occurs early in life when there is so much growth occurring.
There have been many different techniques proposed for the way the foot is manipulated and the way the casts are applied. Treatment of the infant with clubfoot is definitely one of the arts of medicine. Successful treatment requires patience and attention to detail.
The success of treatment of clubfoot by manipulation and casting alone varies greatly. The majority of infants will eventually require surgery but the manipulation and casting begins the process of guiding the foot towards a more normal form. In the infant that eventually needs surgery, the manipulation and casting are still required to obtain as much correction as possible prior to the surgery.
Surgery
When it is clear that manipulation and casting alone will not result in success, your surgeon will recommend surgery. The main question is when to perform the surgery. The earlier the surgery is performed, the more growth that remains in the foot. The more growth remaining, the more the deformity can be corrected. The downside is that a smaller foot is much harder to effectively operate on and the risk of damage to the nerves, blood vessels, and bones is much higher.
Most surgeons recommend waiting until the foot is about eight centimeters (three inches) long. This usually occurs when the infant is about nine months old. Most surgeons agree that it is ideal to have the surgery over and healed before the infant starts to try and walk. Surgery performed at nine months will usually accomplish this goal.
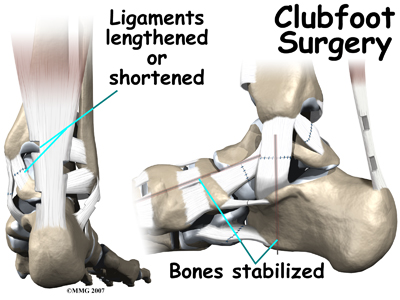
The surgical procedure to correct clubfoot is tedious and complex, but the goals are always the same. Your surgeon will find and cut all the ligaments that are too tight. When they are cut, they eventually heal back with scar tissue. In the growing infant, this scar tissue will grow back to form new ligaments that are not so tight.
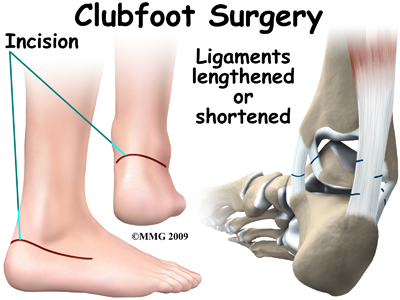
Once the ligaments have been loosened, your surgeon can align the bones of the foot as normal as possible. Metal pins are commonly used to hold the bones in the proper alignment. These metals pins stick out through the skin and are removed three to six weeks after the surgery is completed.
After Surgery
After surgery for clubfoot, a large bandage is applied to the foot. Some type of cast or brace may also be used. The child will probably need to wear some type of brace for several months, and maybe even years after the surgery, but ideally, the treatment should not interfere with the normal developmental milestones. Once the surgery is over, Mother Nature takes over. Weight bearing will help guide the growth in the foot towards a more functional orientation where the sole of the foot can be placed flat on the floor. Physical therapy at Miller PT can be very helpful as well in improving the functional use of the foot.
Rehabilitation
What should be expected from treatment?
Physiotherapy at Miller PT after surgery for a clubfoot can begin as soon as your child’s surgeon recommends it. All treatment, either surgical or non-surgical including physical therapy, is designed to give the child a foot that can be placed flat on the floor. Another goal of therapy at Miller PT is to assist your child’s walking biomechanics in order to encourage your child to walk as efficiently as possible. Lastly, our goals also include relieving any pain if present, preventing pain in the future, maintaining the flexibility of your child’s muscles and tissues, and preventing any weaknesses around the lower extremities and core from developing.
During your first appointment at Miller PT your physical therapist will discuss your child’s foot brace with you and ensure that you are confident putting it on and taking it off. Your doctor will set the specifications of the brace according to your child’s needs. Your doctor will inform you which activities are safe while in the brace and which ones should be avoided. Your child must learn that he/she can kick and swing the legs simultaneously with the brace on. If your child is still young, your physical therapist can help you learn how to hold and handle your child with their brace on. If your child is old enough, they should be encouraged to be part of the routine of putting the brace on and taking it off. General bracing advice, such as the best types of socks and clothing garments to wear with the brace as well as proper strapping or lacing of the brace will also be discussed.
Your physical therapist will also inspect your child’s bare feet and note any areas of the brace that may be irritating your child. Generally your child will need to build up a tolerance to wearing the brace and for this reason some areas where pressure is noted by redness may be considered normal. Any areas of redness, however, should be closely monitored and padded for extra comfort and to disperse the pressure if necessary.
Creams or lotions should not be applied to areas where the skin is red (and unbroken) as this can make the friction worse. Areas that have developed blisters will need to be protected to avoid them getting worse or breaking open. Any broken or fragile skin can become a more serious problem and prevent the braces from being worn for a prolonged period of time, which can result in a relapse of the clubfoot position. In some cases a return visit to your doctor or Orthotist for an early adjustment of the brace may be necessary.
The schedule of how long your child will have to wear the brace each day will be set by your child’s surgeon. At first the time with the brace on will likely need to be most of the day and night. Generally the wearing time is gradually decreased over time so that your child has some awake time without the brace on. In most cases children will need to wear the brace during all sleep times until eventually sleep time is the only time the child is required to wear the brace. Depending on the age of your child, once the brace is discarded during the day, your physical therapist may incorporate taping techniques of the foot to provide gentle foot positioning guidance.
Your physical therapist may address any pain issues that your child may be experiencing from the surgical procedure or the deformity itself, depending on the age of your child. Your physical therapist may use modalities such as ice, heat or massage to try to relieve any pain. In some cases they may even use ultrasound, again depending on your child’s age and the location of their pain.
Maintaining the length of the tissues in your child’s foot is the main goal of any stretching exercises we do with your child or ask you to do with them. Your child’s age at the time of surgery will largely influence how formal the stretches and strengthening exercises for your child will be. If they are old enough to understand and follow along, your physical therapist may encourage specific stretches for the back of the calf and Achilles tendon, as well as for the bottom of the foot. Often, however, children who have had surgery for clubfoot are too young to effectively engage in formal stretches therefore play activities that encourage these types of stretches will be taught. Ensuring that your child spends time squatting, standing with feet flat, standing on their toes, standing on their heels, walking without the brace, and practicing jumping are ways to encourage proper foot movement. Your physical therapist will guide you through which of the activities are most important for your child at which time, the proper technique for these activities, and how long they should be performing each activity. While at Miller PT you will be taught by your therapist how to apply pressure properly to your child’s foot or leg during these activities in order to encourage normal foot alignment. If your child is too young to walk or do the higher level activities then your physical therapist will teach you age-appropriate play activities that encourage the proper positioning of your child’s foot and lower leg. Range of movement exercises that encourage motion of the foot in all directions away from the clubfoot position will be important. Of particular importance are passive Achilles tendon stretches, which will be taught to you and will be encouraged frequently. The Achilles tendon is the thick tendon at the back of the ankle.
Maintaining the length of the Achilles tendon after casting and surgery to lengthen it prepares the foot and ankle to take the body’s weight for activities such as walking, squatting, and jumping. It should be noted how important it is to maximize use of the time that your child spends outside of the brace by doing the specified activities that your physical therapist prescribes as this will train the muscles to hold your child’s new foot position and give the other tissues as much active stretching as possible.
Formal strengthening exercises for older children will be taught which encourage ankle, calf, hip, and core strengthening as well strengthening for the muscles that pull the foot into a position where the sole of the foot is turned up and out (opposite to the clubbed foot position.) As previously mentioned often the child who has had surgery for clubfeet is too young to perform any formal exercises. Playing is once again the best method to encourage strength development in your child’s feet, legs and core area.
Your physical therapist will encourage fun play activities and games such as assisted frog jumps or hops on one leg in order to strengthen the appropriate muscles. Even helping the young child mimic these types of activities can be very useful to strengthen the legs and feet and encourage proper foot position. Any activity they enjoy which encourages the proper motion is useful! Often singing while doing activities or making a game of the exercises is the best method of incorporating rehabilitation into your young child’s world.
For those children that are old enough to ambulate, gait retraining when the brace is off is a crucial part of our rehabilitation at Miller PT after surgery for clubfeet. By using hands on techniques your therapist will encourage the appropriate motions for your child while they walk and they will teach you how to do the same for when you do the exercises at home. Your physical therapist will also work on your child’s foot and ankle proprioception (knowing where their foot is in space without them having to look at it) by having them stand or walk on different surfaces such as a soft mat or foam, as well as on different angles. Activities such as hopping or climbing on apparatus will also help to improve their proprioception. Climbing up onto things such as stairs or gym equipment simultaneously helps to build the needed strength in the hip area, which is an important area that assists in controlling the knee and foot position. For children who are not yet walking, holding them in the standing position (with proper foot alignment) on different surfaces as well as on different angles will accomplish the same thing. Most importantly, for all exercises, the goal is to get the foot into a proper weight bearing position and keep it out of the clubbed foot position.
Your therapist will be a useful resource for discussing footwear modifications for your child if needed. They may consult with a Podiatrist to ensure that the most appropriate footwear is prescribed for you child.
As your child grows, rehabilitation will need to be continued but the frequency of sessions should decrease as long as early intervention has started your child on the right path to correcting the alignment of your child’s foot, ankle, and lower limb, and as long as you are actively doing the home rehabilitation program. As your child grows and becomes more mature, physical therapy at Miller PT will include more formal types of exercises to encourage proper foot alignment. It is expected that your child will eventually be able to partake in all physical activities that other children their age partake in.
Generally children who have had surgery for clubfeet do extremely well with the physical therapy we provide at Miller PT. Over the course of your child’s therapy your therapist will liaise closely with your child’s doctor, surgeon, Orthotist, and Podiatrist as well as any other health care professionals that are involved in their care to ensure your child is recovering as quickly and normally as possible.
Miller PT provides services for physical therapy in Delray Beach.
Complications
What can go wrong?
As with any treatment, complications can result from both conservative and surgical treatment of clubfoot. Failure of manipulation and casting to result in a successful outcome is not a complication. The majority of patients will not be treated successfully with non-surgical treatment alone.
Several complications are possible both during and after surgery. Wound problems may occur after surgery due to abnormal swelling or pressure from the cast. When the foot is markedly deformed, correction of the deformity may stretch the skin so tight that the blood supply is compromised. This may result in a small section of the skin actually dying. This normally heals with time and only rarely does this require a skin graft.
Infection can occur following any type of surgery. A wound infection can occur after clubfoot surgery. This may require additional surgery to drain the infection and antibiotics to treat the infection.
The infant foot is very small. The structures are very difficult to see even using magnifying glasses. Blood vessels and nerves may be damaged or cut during the operation. The bones of the infant foot are mostly made of cartilage. This material can be damaged, resulting in deformities of these bones. This damage usually corrects itself with growth.
Up to half of all patients undergoing clubfoot surgery will require at least one additional surgical procedure later in life.
Portions of this document copyright MMG, LLC







